
 Obviously, care for the human heart is implied for any living person, but especially so for athletes. But, what does a healthy heart mean? What makes up an unhealthy heart? And how can an unhealthy heart masquerade as a healthy one leaving someone in serious risk. Being one of the most fascinating systems in the human body, I thought I would take a moment to explain it in the context of the endurance athlete.
Obviously, care for the human heart is implied for any living person, but especially so for athletes. But, what does a healthy heart mean? What makes up an unhealthy heart? And how can an unhealthy heart masquerade as a healthy one leaving someone in serious risk. Being one of the most fascinating systems in the human body, I thought I would take a moment to explain it in the context of the endurance athlete.What is a healthy heart?
Hearts are monitored with regard to physical stature and mechanics. Clearly for a heart to be effective, it must beat (beware, link contains surgical footage), but a beating heart alone does not imply a healthy system. For the heart to beat, a highly sophisticated electrical and mechanical system must operate in perfect rhythm. When assessing the health of this system, rate and rhythm are taken into account. Rate, basically are measured in beats per minute. However, rate does not imply rhythm, and a heart beating a 68 bpm may have a dangerously erratic rhythm. Healthy hearts operate under what is known as sinus rhythm which gets its name from the electrical "pacemaker" of the heart, the sinoatrial node. Under the proper operation of this node, the heart clips along at a regular and predictable rate, only varying slightly by pressure exerted on the heart by the lungs during inhalation.
Road Map of the Heart:
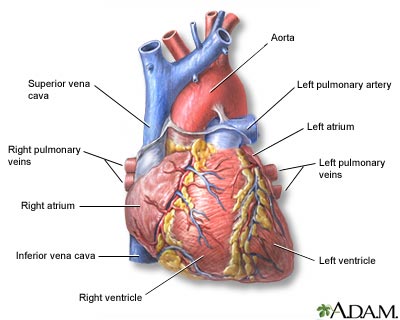
The heart consists of four chambers: two atrium, and two ventricles. The atrium and ventricles are pair respectively as "right" and "left". Between these pairs are a sophisticated one way valve allowing blood only to travel from atrium --> ventricle and not in reverse. That is the basic make up of the structure of the heart itself, but leading into and out of each chamber are curtain vessels. The most important of these is the Aorta (leading out of the left ventricle to the body) and the Pulmonary Artery (leading out of the right ventricle to the lungs). Also coming into the right atrium are the superior and inferior Vena Cava. There are other smaller vessels, but for simplicity these are the major players.
If you followed one blood cell as it travels up the veins in, say, the leg it would travel up through the Inferior Vena Cava to the right atrium, then down to the right ventricle where it is pumped up the Pulmonary Artery to the lungs where the blood is oxygenated. From there it travels into the left atrium through the Pulmonary Vein and then enters the left ventricle where it is pumped out through the Aorta and out to the systemic body.
What is "Lub-Dub":
Everyone knows the lub-dub, lub-dub, lub-dub they hear in their chest. But what are those sounds? In medicine Lub is known as the 1st heart sound (S1) and Dub is the second (S2). There are four total hearts sounds (S3, S4) but the 3rd and 4th are pathological and usually indicated disease, meaning you won't hear them in a healthy heart. But what ARE the sounds? Lub is the sound of the tricuspid and mitral valves between the atrium and ventricles basically slamming shut. This is due to the ventricle contracting and the pressure pushing the valves closed so blood doesn't travel backwards to the atrium. Dub is the sound of the aortic and pulmonic valves closing in response to back-pressure from the body. When the ventricles finish contracting, they are pushing against a wall of pressure in the body (blood pressure). When the contraction is done the pressure wants to push blood back in the heart as it re-expands. The aortic and pulmonic valves flare open and allow this not to happen. What is more interesting is the Aorta in this case. Most think of it as a inanimate vessel, but it actually has a contractive function that is timed with the heart to squeeze blood away from the center to the periphery.
Fun Fact: If you put your ear to someone's chest, or listen to your own with a stethoscope you can physically "split" your 2nd heart sound. You do this by taking a deep breath. This causes the aortic valve and pulmonic valve to close at slightly different times giving a sound like "lub-da-dub". This is caused by both increases structural pressure on the heart from the lungs and an increase in blood pressure in the pulmonary system causing the pulmonic valve to become more reactive.
Myocardium:
Myocardium (myo: muscle, cardium: heart) is one of only three muscle types found in the entire body. It's make-up and function are so specific that it sets it apart from the other two entirely. It most closely resembles skeletal muscle in make up, but is equipped with function and energy to operated constantly, something skeletal muscle is not set up to do. This high level of function has a high energetic demand from the body system. Enormous amounts if oxygen are needed to preserve that function and oxygen supply IS blood supply. Oxygen is delivered through the coronary arteries to the myocardium.
Electricity:
 The electrical system responsible for conducting the heart may be the most fascinating part of the system simply because it is required to be so reliable. Impulses from the central nervous system reach the heart at the sinoatrial node (SA). From there an impulse is transmitted through the atrium stimulating their contraction. Impuses from the SA node travel to another node between the atrium and ventricles called the Atrioventricular node (AV). This node then signals the contraction of the ventricles. The fascinating part of this system is that it is designed to operated on a delay so the atrium contract slightly before the ventricles. This keeps the system pumping "forward".
The electrical system responsible for conducting the heart may be the most fascinating part of the system simply because it is required to be so reliable. Impulses from the central nervous system reach the heart at the sinoatrial node (SA). From there an impulse is transmitted through the atrium stimulating their contraction. Impuses from the SA node travel to another node between the atrium and ventricles called the Atrioventricular node (AV). This node then signals the contraction of the ventricles. The fascinating part of this system is that it is designed to operated on a delay so the atrium contract slightly before the ventricles. This keeps the system pumping "forward".Cardiac Output:
Cardiac Output (CO) is the overall measure of the pump function of the heart. The equation CO=Heart Rate (HR) x Stroke Volume (SV) best explains the overall potential of the heart. This is helpful in understanding why certain people have differing heart rates, and output potentials. The phenomenon known as "Athlete's heart" is basically a non-pathologically oversized heart ( pathologically over sized hearts, or Hypertrophic Cardiomyopathy will be discussed in part 2 of this post ). Basically the heart in an athlete has developed so well, that it has an enormous stroke volume (SR). If you plug a high figure into the above equation, then to get the same overall cardiac output you require a much smaller number out of the heart rate (HR), thus the reason why athletes have such remarkably low heart rates! Some marathon runners regularly have HR in the mid 30's. That means their hearts is about twice as effective at pumping blood as the average person. On the flip side, people with failing hearts and low SV in turn must have very high heart rates to equal the required CO.
Cardiac Output changes as the demand from exercise increases. Since the SV changes very little when exercising, the HR must increase to meet the new CO requirements of the body.
Max HR:
This is the figure that determines your max heart rate before the heart is no longer able to feed itself properly to function and begins to be damaged. Originally the number was determined by the calculation of 220-age for males and 226-age for females, with the stipulation that this varied from person to person quite a bit. However, it's been found that this is not a reliable predictor, so other equations came out to try to make more accurate the prediction possibilities. Truth be told the only way to truly determine your Max HR is to undergo a cardiac stress test. Since few actually go this route, this can be a little dangerous because Max HR is often the baseline for determining exercise programs. My opinion is be conservative on this number, especially for beginners.
Optimal HR:
Optimal HR is even more dependent on the specific person that Max HR. This depends on how fit a person is, and what they desire to get out of working out the heart. There are basic % breakdowns of Max HR (as calculated by 220-age) that determine which phase the heart is in, and which benefit it will gain from operating in this range. Basically the most important mark is around 80% of Max HR, which is the point at which the heart is no longer operating aerobically and goes into anaerobic function (meaning the system no longer able to meet the oxygen demand of the heart) There are specific reasons to work within that range of anaerobic function, but this should be highly regulated because it is easy to begin damaging the heart at this point. Generally, for fat burning exercise operating within 70-80% of Max HR is optimal, and for general health and endurance operating under 65% is best. Again these numbers vary significantly!
Understanding your own heart's potential is crucial in creating an exercise program designed to enhance performance.
The next post will be on the unhealthy heart, disease and understanding causes and avoidance of heart disease.


{kind=link}
{kind=link}
{kind=link}
1 comment:
Well, our entire Miracle Team must have "athlete's hearts", because I've never met a bunch of people with more passion, more love, or more support for fellow teammates than this crowd.
Love you all. Looking forward to rain rides, night rides, fun rides, and race rides...
Great post, Jess. I'll read carefully your next post on the unhealthy heart ;)
Post a Comment